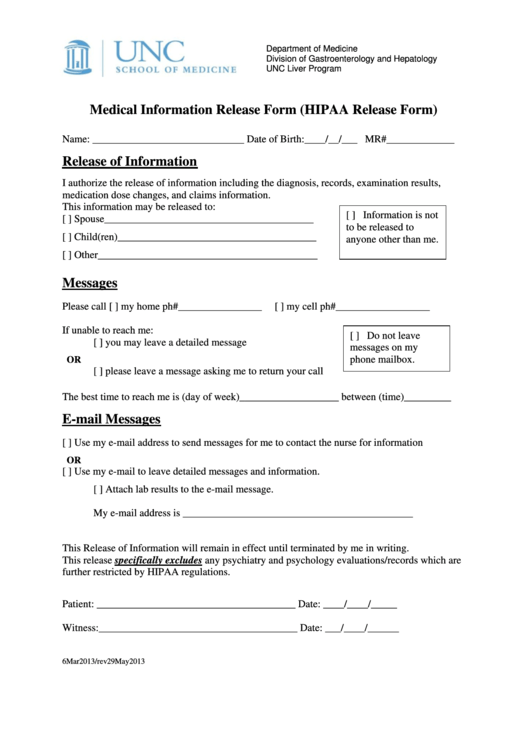
Unc Medical Release Form - 07/2019 page 2 of 3 chart location: Unc hospitals health information management attn: If you want to mail your request or drop it off in person, you’ll need to download and fill out the authorization form for medical records. Please check if you wish to authorize the release of sensitive medical information: Find the address for your provider’s office and mail, fax,. I must revoke this authorization in writing. ☐ mental health/psychiatric treatment ☐ genetic testing information alcohol or substance abuse. Please send your completed authorization form to: My initials below authorizes inclusion of information pertaining to: Authorization forms i hereby release unc health care system and its affiliates and employees from any and all liability that may arise from.
If you want to mail your request or drop it off in person, you’ll need to download and fill out the authorization form for medical records. 07/2019 page 2 of 3 chart location: Please check if you wish to authorize the release of sensitive medical information: ☐ mental health/psychiatric treatment ☐ genetic testing information alcohol or substance abuse. The procedure for revoking this authorization is to present my. I must revoke this authorization in writing. Please send your completed authorization form to: Find the address for your provider’s office and mail, fax,. My initials below authorizes inclusion of information pertaining to: Release of information 600 eastowne drive, 3rd floor chapel hill, nc 27514.
If you want to mail your request or drop it off in person, you’ll need to download and fill out the authorization form for medical records. Release of information 600 eastowne drive, 3rd floor chapel hill, nc 27514. Authorization forms i hereby release unc health care system and its affiliates and employees from any and all liability that may arise from. The procedure for revoking this authorization is to present my. Unc hospitals health information management attn: My initials below authorizes inclusion of information pertaining to: ☐ mental health/psychiatric treatment ☐ genetic testing information alcohol or substance abuse. 07/2019 page 2 of 3 chart location: I must revoke this authorization in writing. Find the address for your provider’s office and mail, fax,.

Best Authorization To Release Medical Records Guide 2024 Guide
Please send your completed authorization form to: I must revoke this authorization in writing. Please check if you wish to authorize the release of sensitive medical information: Unc hospitals health information management attn: Release of information 600 eastowne drive, 3rd floor chapel hill, nc 27514.
This item is unavailable Etsy
07/2019 page 2 of 3 chart location: ☐ mental health/psychiatric treatment ☐ genetic testing information alcohol or substance abuse. Release of information 600 eastowne drive, 3rd floor chapel hill, nc 27514. I must revoke this authorization in writing. Please send your completed authorization form to:

Uc Davis Authorization To Release Information Form
I must revoke this authorization in writing. 07/2019 page 2 of 3 chart location: Find the address for your provider’s office and mail, fax,. My initials below authorizes inclusion of information pertaining to: Unc hospitals health information management attn:
Unc Medical Records Release Form
Unc hospitals health information management attn: The procedure for revoking this authorization is to present my. Authorization forms i hereby release unc health care system and its affiliates and employees from any and all liability that may arise from. My initials below authorizes inclusion of information pertaining to: If you want to mail your request or drop it off in.
Medical Release Form Template Business
Please send your completed authorization form to: My initials below authorizes inclusion of information pertaining to: Authorization forms i hereby release unc health care system and its affiliates and employees from any and all liability that may arise from. Please check if you wish to authorize the release of sensitive medical information: Unc hospitals health information management attn:
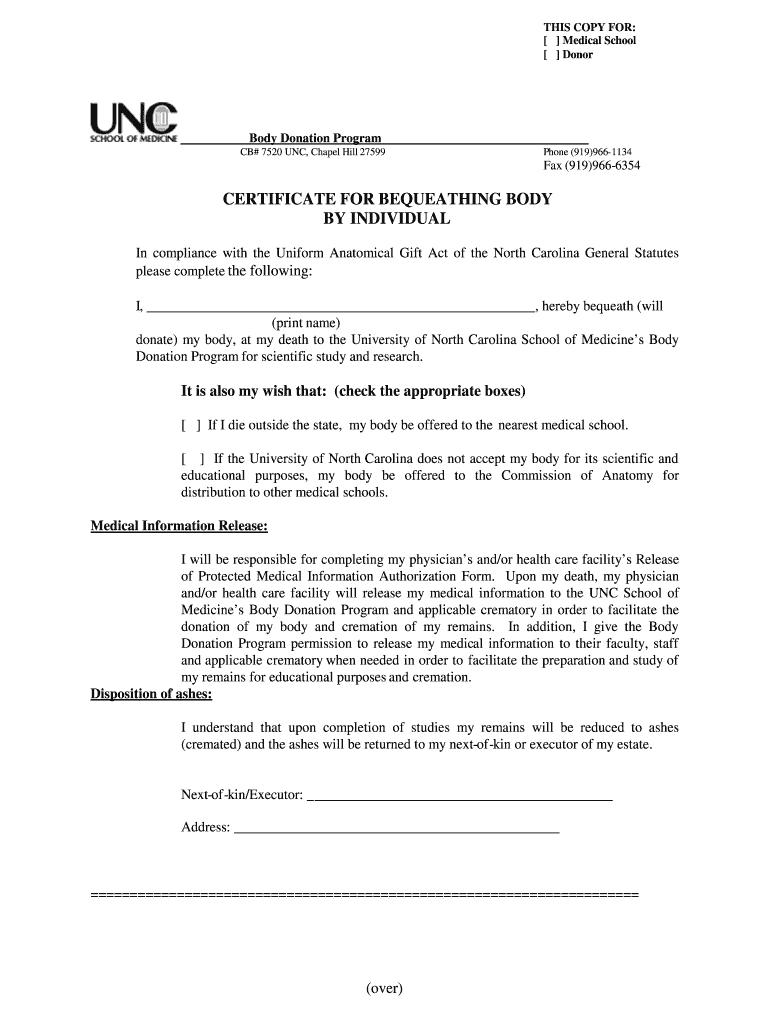
Unc Body Donation 20072024 Form Fill Out and Sign Printable PDF
Authorization forms i hereby release unc health care system and its affiliates and employees from any and all liability that may arise from. If you want to mail your request or drop it off in person, you’ll need to download and fill out the authorization form for medical records. Please check if you wish to authorize the release of sensitive.

Unc Rex Medical Records Fill Online, Printable, Fillable, Blank
The procedure for revoking this authorization is to present my. Find the address for your provider’s office and mail, fax,. If you want to mail your request or drop it off in person, you’ll need to download and fill out the authorization form for medical records. Authorization forms i hereby release unc health care system and its affiliates and employees.

Nc Hd Authorization Fill Online, Printable, Fillable, Blank pdfFiller
The procedure for revoking this authorization is to present my. ☐ mental health/psychiatric treatment ☐ genetic testing information alcohol or substance abuse. My initials below authorizes inclusion of information pertaining to: Please send your completed authorization form to: Authorization forms i hereby release unc health care system and its affiliates and employees from any and all liability that may arise.
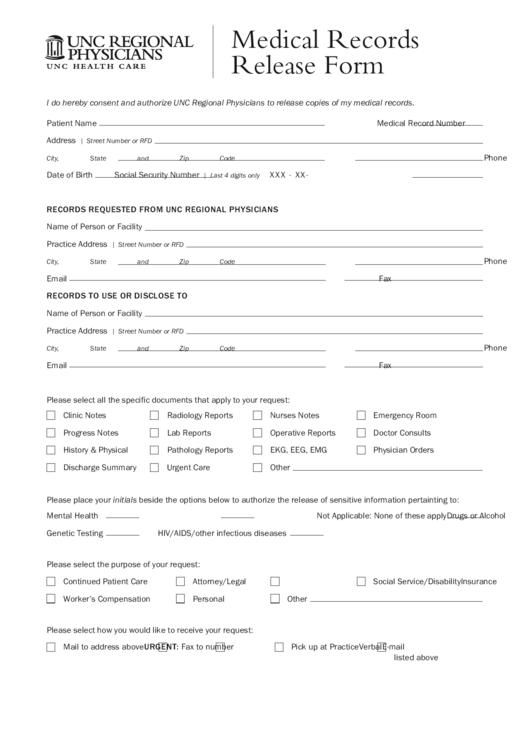
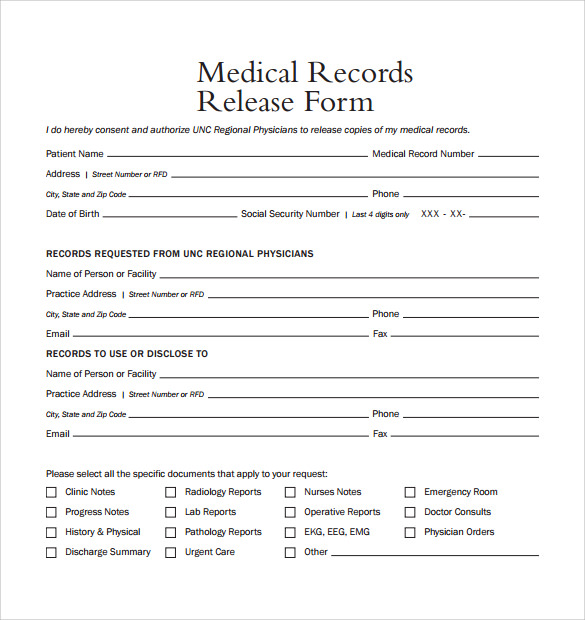
Unc Regional Physicians Medical Records Release Form printable pdf download
Please send your completed authorization form to: 07/2019 page 2 of 3 chart location: Unc hospitals health information management attn: I must revoke this authorization in writing. Authorization forms i hereby release unc health care system and its affiliates and employees from any and all liability that may arise from.

UNC Hospitals Lands Spot on List of Nation's Best Cancer Facilities
☐ mental health/psychiatric treatment ☐ genetic testing information alcohol or substance abuse. If you want to mail your request or drop it off in person, you’ll need to download and fill out the authorization form for medical records. Please check if you wish to authorize the release of sensitive medical information: Please send your completed authorization form to: 07/2019 page.
07/2019 Page 2 Of 3 Chart Location:
☐ mental health/psychiatric treatment ☐ genetic testing information alcohol or substance abuse. Please check if you wish to authorize the release of sensitive medical information: Please send your completed authorization form to: If you want to mail your request or drop it off in person, you’ll need to download and fill out the authorization form for medical records.
The Procedure For Revoking This Authorization Is To Present My.
Release of information 600 eastowne drive, 3rd floor chapel hill, nc 27514. Authorization forms i hereby release unc health care system and its affiliates and employees from any and all liability that may arise from. My initials below authorizes inclusion of information pertaining to: I must revoke this authorization in writing.
Unc Hospitals Health Information Management Attn:
Find the address for your provider’s office and mail, fax,.