Orthodontic Release Form - Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.
I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest.
Orthodontic treatment requires the full cooperation of the. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.
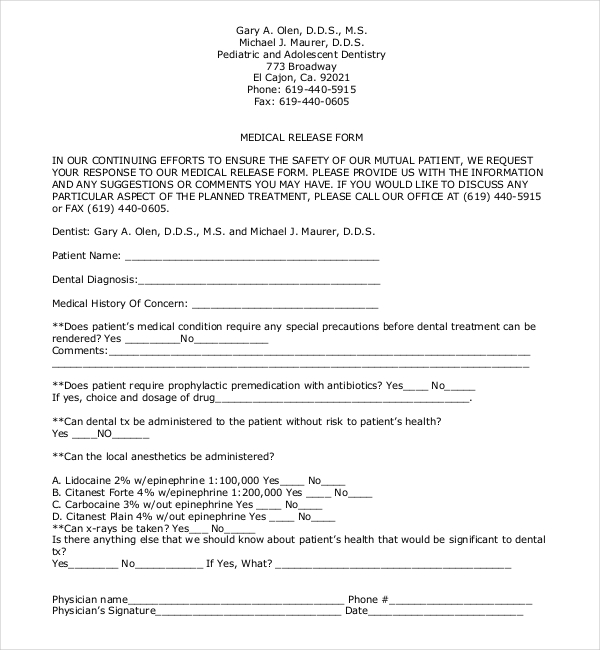
FREE 22+ Sample Medical Release Forms in PDF Word Excel
Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. I further acknowledge that said doctor has advised me against removal of said appliances at this time,.
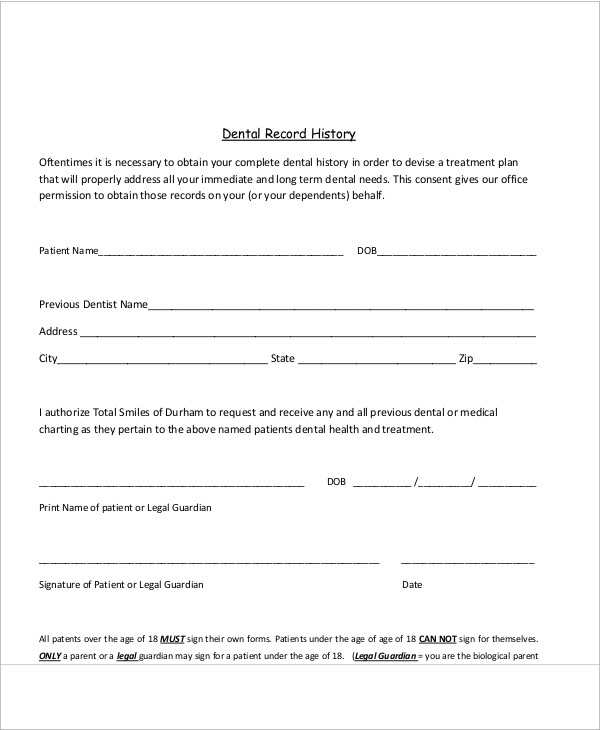
FREE 11+ Sample Dental Release Forms in MS Word PDF
Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,.
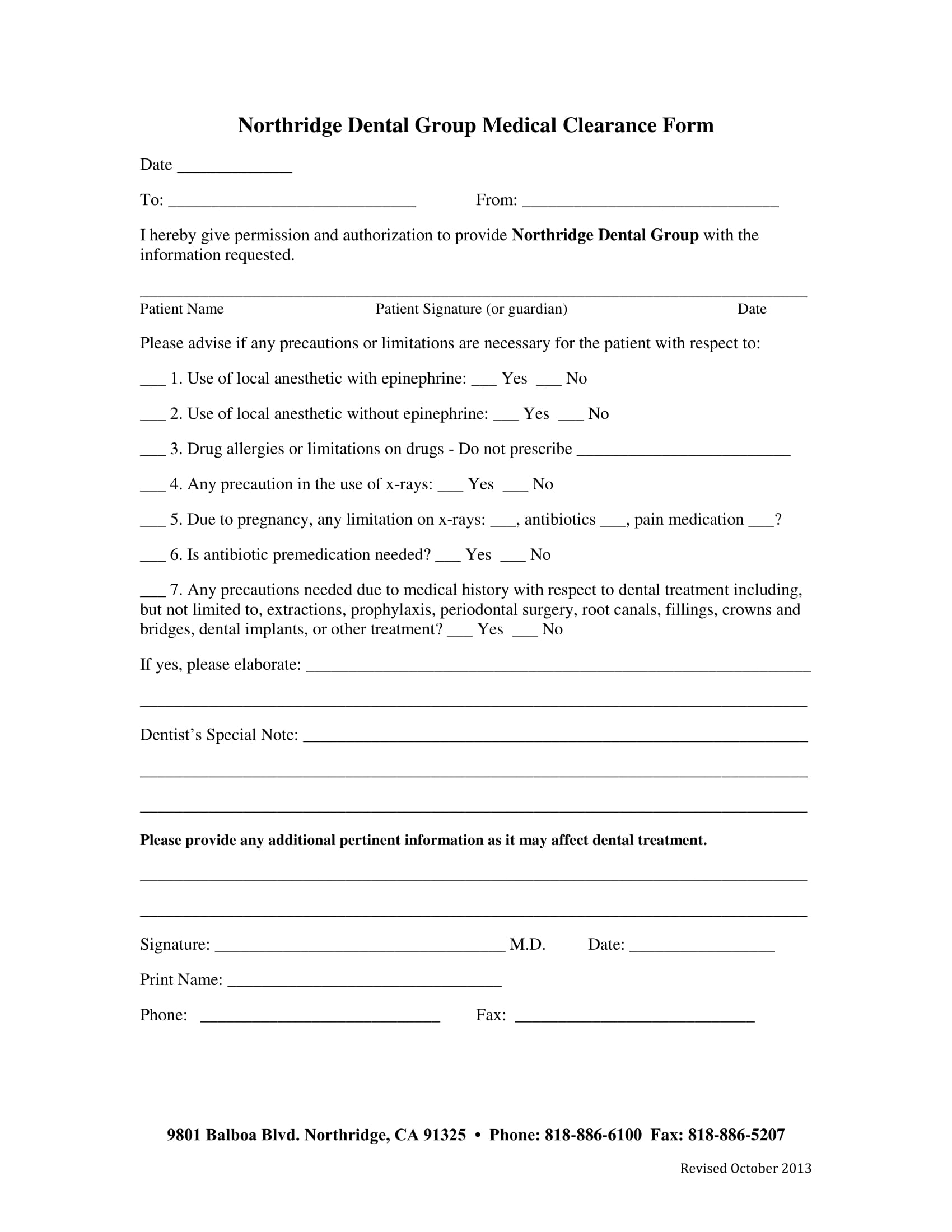
Printable Medical Clearance Form For Dental Treatment
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.
FREE 11+ Sample Dental Release Forms in MS Word PDF
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the.

Concerns About Your Child's Ortho Health Prettyman Orthodontics
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest.
Early Removal Of Braces Consent Form Fill Online, Printable, Fillable
I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest.
Aao Transfer Form Printable Printable Forms Free Online
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.

Dental XRay Release Form Template Word PDF Google Docs Highfile
Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Orthodontic treatment requires the full cooperation of the.
FREE 6+ Dental Records Release Forms in PDF MS Word
I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,.

Authorization To Release Dental Information Printable Pdf Download
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.
Orthodontic Treatment Requires The Full Cooperation Of The.
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest.